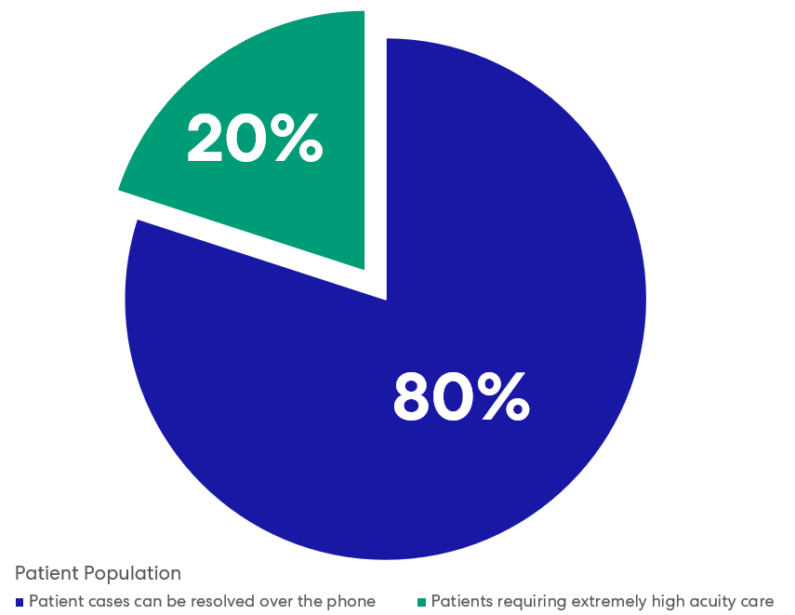
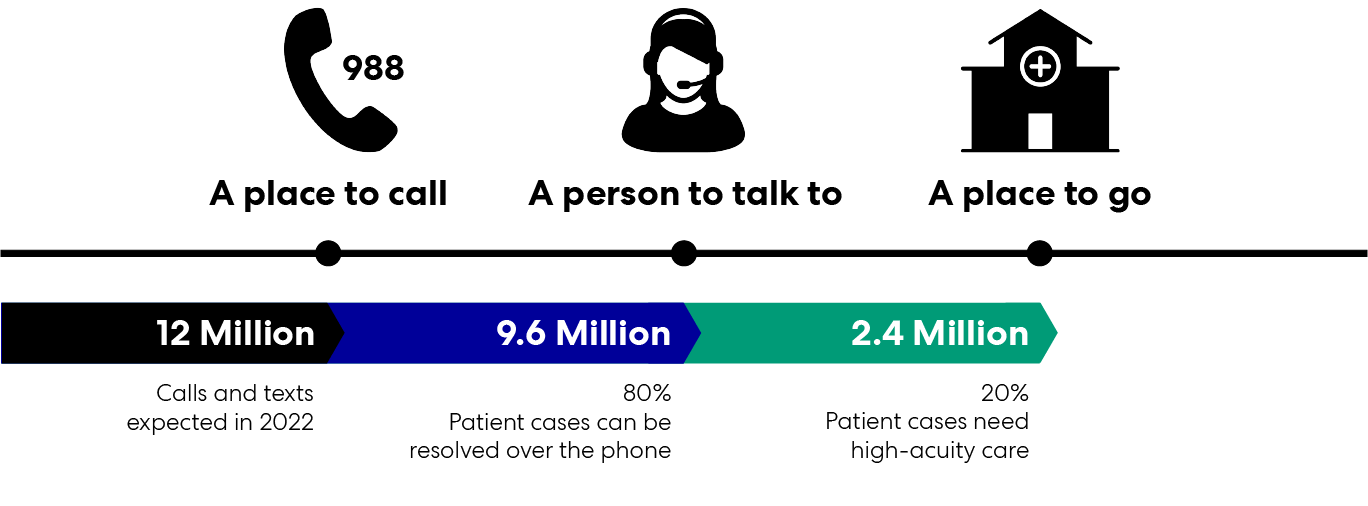
The national Suicide and Crisis Lifeline, 988, went live on July 16. We now have a new dedicated national telephone number that we can call or text anytime when a mental-health crisis arises for ourselves, our loved ones, or people in our communities.
Perspectives
July 22, 2022
988 is here: it’s time to respond
Healthcare Design for a Comprehensive Continuum of Care